Physical Therapy Medical History Form
Download printable Word doc - Medical History Form Download printable PDF - PDF Patient Medical HistoryPatient Medical History
Patient Name _______________________Date _______________
Are you presently working? □ Yes □ No
Date of next physicians visit _______________
1. Date of injury/Onset _______________________
2. Have you ever had these symptoms before □ Yes □ No
3. Check all that apply to your symptoms:
□ Work related injury □ Reoccurrence of previous injury □ Motor vehicle accident
□ Injury related to lifting □ Athletic or recreational injury □ Cause unknown
□ Other_____________________________________________________________________
Have you had a related surgery? □ Yes □ No when: ___________________________
Do you currently have or have had in the past any of the following?
□ Heart Attack □ Heart Disease □ Heart Palpitations □ Chest Pain Angina
□ High Blood pressure Are you on blood thinners □ Yes □ No Pacemaker □ Yes □ No
□ Diabetes □ Type 1 juvenile □ Type 2 Adult onset □ Do you take insulin?
□ Asthma/Breathing Difficulties Do you use a rescue inhaler □ Yes □ No
Are you pregnant? □ Yes □ No Do you smoke? □ Yes □ No
□ Headaches □ Dizziness/Fainting □ Ringing in your ears □ Seizures
□ Kidney problems □ Cancer □ Hernia □ Special diet guidelines
□ Bowel/Bladder abnormalities □ Liver/Gallbladder problems
□ Allergies to aspirin □ Allergies to heat □ Allergies/poor tolerance to cold
□ Recent fractures □ Recent Surgery □ Metal implants □ Rheumatoid arthritis
□ Skin abnormalities □ Sexual dysfunction □ Nausea/Vomitting
□ Other_______________________________________________________________
_______________________________________________________________
Patient Medical History
Patient Name ______________________________ Date _______________
If you answered yes to any of the previous questions – please explain and give approximate date:
Is there any other information regarding your past medical history we should know about?
________________________________________________________________________________________
_______________________________________________________________________________________
Are you currently taking any medications? □ Yes □ No If so – please list below
What is the intensity of your pain on a scale of 1 to 10. With 0 being
In the rare instance of an emergency who should we contact?
Name _____________________Phone ___________________
Do you participate in any sport, activities, or exercise program on a regular basis □ Yes □ No
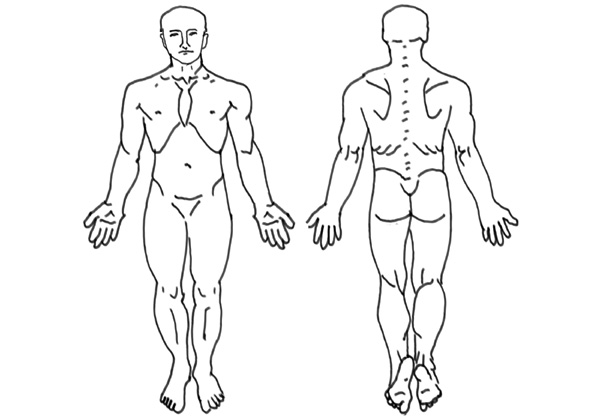 Please show us where your pain is on the illustration above
Please show us where your pain is on the illustration above